CP/Swallowing/Treatments
Cerebral palsy may involve muscle stiffness (spasticity), poor muscle
tone, uncontrolled movements, and problems with posture, balance, coordination, walking, speech, swallowing, and many other
functions. There is no specific cure for cerebral palsy, but proper management helps to reduce complications and maximize
functional independence. Physical and occupational therapy can enhance motor skills; braces, splints, casts, or orthopedic
surgery may improve the function of the limbs; mechanical aids; management of spasticity with medications, injections or surgery;
medicated seizure management; and feeding tubes for severe swallowing impairment are the general areas of treatment for cerebral
palsy.
Poor nutrition is often a major concern of individuals with cerebral
palsy, due to motor deficits in the oral cavity. This, in turn, may make the individual more susceptible to infections,
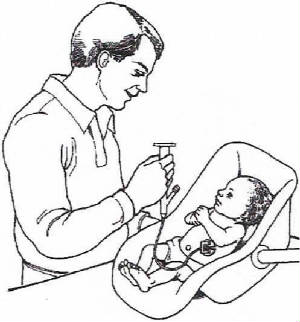
which could lead to additional delays in growth and development. To aid in the swallowing process, semisolid foods,
such as strained vegetables and fruits may be recommended. Proper position, such as sitting up while eating or drinking
and extending the individual’s neck away from the body to reduce the risk of choking is beneficial.
Inadequate control of the muscles of the pharynx, oral cavity, and
tongue may also lead to drooling. Drooling is a problem for approximately 10% of individuals with cerebral palsy and
presents health and cosmetic issues. (Jongerius et. al, 2004). Many of those affected by this consider it their worst affliction because of embarrassment and social isolation.
Excessive drooling can also cause skin lesions, yeast infection, salivary aspiration, and dehydration. Interventions
may include oral motor stimulation therapy, behavioral modification, stylish scarves, medications, botulinum-toxin injections,
oral appliances, or surgery (Cooley,2004). Medications can reduce the flow of saliva but may cause significant side
effects, such as mouth dryness and poor digestion. Surgical approaches, include removal of the submandibular gland,
cutting or rerouting the salivary duct, and nerve removal, have been used with varying results.
Children with Cerebral Palsy can usually be placed into
three categories of swallowing disorders:
(1) those with moderate to severe oral function problems, including
reduced lip closure and tongue thrust, as well as reduced tongue coordination;
(2) those with the same moderate to severe oral problems and
a delay in triggering the pharyngeal swallow;
(3) those with moderate to severe oromotor problems; pharyngeal
delay, and neuromuscular abnormalities in their pharyngeal swallow, including reduced tongue base retraction and reduced laryngeal
elevation, resulting in significant residue in the pharynx after the swallow and increased risk of aspiration after the swallow”
(Logemann, 1998).
Many children with CP exhibit an array of oral problems, including
tongue thrust, inadequate lateralization of the tongue and uncoordinated anterior to posterior movement. They also exhibit
a delay in triggering the pharyngeal swallow.
Management strategies may include oral motor therapy, thermal-tactile
stimulation of the pharyngeal swallow, and diet change, including thickened liquids and purees (Logemann, 1998).
Diet change should be the last choice for management because it
is less appealing to the child and the family. The swallowing therapist should identify the most advantageous therapy
and eating strategies, educate the caregivers, and frequently supervise the caregivers.
Cricopharyngeal Myotomy
Cricopharyngeal dysfunction or abnormal opening of the upper esophageal
sphincter is an infrequent, but possible problem in an individual with cerebral palsy and could be an issue. In this
case, a cricopharyngeal myotomy may need to be considered as a last resort following swallowing therapy.
“This procedure involves an external incision through the
side of the neck (usually the left side) into the cricopharyngeal muscle, slitting the fibers of the muscle from top to bottom,
usually at the posterior midline, to permanently open the sphincter. The incision typically extends upward to include
some of the inferior constrictor fibers, and downward into the esophageal musculature. The patient can usually begin
to eat within 1 week after the myotomy” (Logemann, 1998).
Botulinum Toxin Injection
Botulinum toxin injection therapy (aka “Botox” therapy)
is used to treat dystonia, a neuromuscular disorder that results in involuntary muscle contractions or spasms. It affects
muscles that control movement in the eyes, neck, face, voice box, or the smooth muscle in the bladder. The goal of “Botox”
therapy is a reduction in muscle spasms and pain. Botulinum toxin has proven to be useful in the treatment in oromandibular
dystonia, which is the continuous spasm of the face, jaw, neck, tongue, larynx, and in severe cases, the respiratory system.
In addition, Botox therapy has been known to improve spasmodic dysphonia (spasms in the vocal cords that cause sudden disruption
of speech) and voice tremors. The treatment is usually repeated
every 3 to 4 months, since neurons generate new nerve ending that reactivate the dystonia (Cooley, 2004). Also, some
patients develop antibodies to the toxin over time, making the treatment ineffective.
Furthermore, recent reports have suggested that botulinum neurotoxin type A (BoNT) injections into the salivary glands
as an option for the treatment of drooling (Jongerius et. al, 2004). A study was conducted by Jongerius et. al that
indicated a significant improvement of drooling in 95% of cases after receiving the BoNT injections, according to the subjects’
parents.
Intrathecal Baclofen Therapy (IBT)
Baclofen is a muscle relaxant and antispasmodic that inhibits the
transmission of messages between nerve cells. It is believed that Baclofen replaces the neurotransmitter gamma amino
butyric acid (GABA) that is naturally found in the body. When this chemical is released in the spinal cord the muscles
relax. It can be taken orally, but causes drowsiness and dizziness. A more efficient way to distribute the drug
is by Continuous Intrathecal Baclofen Infusion (CIBI). A pump is inserted under the skin of the abdomen that connects
to a tube that is placed in the spinal canal (Cooley, 2004). This allows the medication to be directly delivered to the
spinal fluid without circulating in the body. Due to computer technology, the medication is delivered in continuous
minute doses. The pump is refilled every one to three months.
The advantage of Baclofen is that it relaxes the muscles that help
with swallowing and speech. The operation lasts about one hour. The doses can be strictly monitored and adjusted
according to the patient’s needs. The pump is typically used in children over the age of 5. However, the
treatment may cause drowsiness and nausea (Cooley,2004). There is also a risk that the pump or surrounding tissues may
become infected.
Tube
Feedings
(1) Nasogastric Tube Feeding:
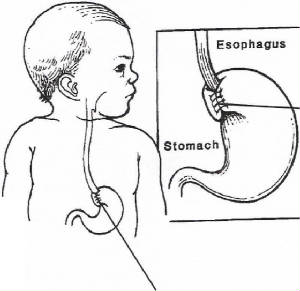
A nasogastric tube is a thin, hollow, soft tube that is passed through
the nose, pharynx, and esophagus into the child’s stomach. For some children, this tube may be passed through
the mouth rather than the nose. The types of NG tubes include: polyvinyl chloride (PVC), silicone, and polyurethane.
Although nasogastric tube-feeding is feasible for extended periods,
children who are likely to require feeding for more than three months should be considered for gastrostomy placement.
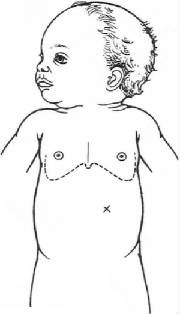
(2) Gastrostomy Tube Feeding:
Gastrostomy feeding in children severely affected
by cerebral palsy can improve nutritional status but does not eliminate growth delays. Gastrostomy tubes are well suited
for long-term enteral feeding. Patient comfort with gastrostomies is an advantage over NG tubes. These tubes do
not irritate the nasal passage, esophagus, or trachea, cause facial irritation, or interfere with breathing. A gastrostomy
tube (GT) is a way to feed babies who are not able to suck or swallow effectively for good nutrition. The gastrostomy
tube is placed directly into the stomach. Their stability and physiologic capabilities permit continued oral eating.
There are button gastrostomies and other skin level feeding tubes
that are easily hidden under a child's clothing. These require less daily care and interfere less with a child's movement.
Gastrostomies use a large-bore tube, which allows a more viscous feedings and decreased risk of tube occlusion.
The
Malecot Catheter, which is a rubber tube, is placed through a hole made in the child’s stomach. The Catheter is
sewn in place until the opening in the skin and stomach jointly heal. It may be removed and replaced with a Foley Catheter
2-4 weeks after the surgery. The tube is kept in place by a special dressing that prevents the tube from being pulled
out.
Occasionally, a Nissen fundoplication is performed at simultaneously
with the gastrostomy tube. This surgical procedure tightens the valve connecting the esophagus and the child’s stomach.
A section of the child’s stomach is wrapped around the esophagus in order to prevent reflux of formula and gastric juices
into the feeding tube or esophagus. Reflux can result in a child spitting up often, esophagus irritation, breathing
problems, or aspiration of formula and/or gastric juices.
Feedings begin slowly about 2 to 3 days post-operation.
Disadvantages of gastrostomy feeding include the surgery required
to place the tube, possible skin irritation or infection around the gastrostomy site, and a slight risk of intra-abdominal
leakage resulting in peritonitis. Of special concern is the child with poor gastric emptying and/or severe reflux or intractable
vomiting. These children have increased risk of aspiration.