What About Treatment?
With early and ongoing treatment the effects of CP can be reduced.
Many children learn how to get their bodies to work for them in other ways. For example, one infant whose CP keeps him from
crawling may be able to get around by rolling from place to place.
Children younger than three years old can benefit greatly from early
intervention services. Early intervention is a system of services to support infants and toddlers with disabilities and their
families. For older children, special education and related services are available through the public school to help each
child achieve and learn.
Typically, children with CP may need different kinds of therapy,
including:
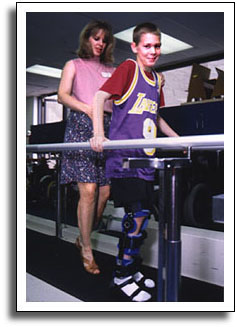
Physical therapy (PT), which helps the child develop
stronger muscles such as those in the legs and trunk. Through PT, the child works on skills such as walking, sitting, and
keeping his or her balance.
Occupational therapy (OT), which helps the child
develop fine motor skills such as dressing, feeding, writing, and other daily living tasks.
Speech-language pathology (S/L), which helps the
child develop his or her communication skills. The child may work in particular on speaking, which may be difficult due to
problems with muscle tone of the tongue and throat.
The child may also find a variety of special equipment helpful.
For example, braces (also called AFOs) may be used to hold the foot in place when the child stands or walks. Custom splints
can provide support to help a child use his or her hands. A variety of therapy equipment and adapted toys are available to
help children play and have fun while they are working their bodies. Activities such as swimming or horseback riding can help
strengthen weaker muscles and relax the tighter ones.
New medical treatments are being developed all the time. Sometimes
surgery, Botox injections, or other medications can help lessen the effects of CP, but there is no cure for the condition.
Electrical Stimulation Therapy
For years Electrical Stimulation (ES) therapy has been used to help muscles regain function. However,
this has generally been associated with sports injuries and Physical therapy. More recently, ES has gained the interests
of Speech therapists for use with those diagnosed with swallowing disorders – or dysphagia. Although still somewhat
controversial within the field of Speech therapy, the use of ES – or a combination of ES and conventional swallowing
therapy – is becoming more and more popular.
How it all began…..
Marcy Freed, Speech therapist and inventor/founder of VitalStim
Therapy – the only electrical stimulation unit approved by the FDA for the treatment of swallowing disorders –
came up with the idea of using ES in 1975 when working with a patient who could not swallow. Being a marathon runner, she
had received ES on several occasions for muscle injuries. She thought if ES could help stimulate and recover function
of muscles used for running, why wouldn’t it help regain function in the muscles involved in swallowing. With a Doctor’s
order, she gained permission to try it on her patient. Within 2 days her patient was eating (Freed, 2006, web).
Based on the success of a study involving 892 in-patients and out-patients from 1993 to 1998, VitalStim received FDA approval.
In order to ensure proper treatment and better outcomes, Speech therapists and other medical professional must be certified
to administer VitalStim therapy. Certification seminars are offered across the country. For more information on VitalStim
or certification seminars, you can visit http://www.vitalstimtherapy.com.
How does it work?
Specially designed electrodes are placed on the anterior portion of
the neck, which deliver a small, carefully calibrated current. Motor nerves in the throat are stimulated, causing the muscles
responsible for swallowing to contract. This improves the swallowing function by strengthening the muscles, increasing
ROM, coordination, and endurance, and, with repeated therapy and functional exercises, “re-educates” the muscles.
The degree and type of swallowing disorder will determine the amount of therapy needed. The average amount of therapy
needed to restore swallowing function is 10 sessions ranging from 30 minutes to 1 hour. However, sometimes it is seen
in as little as 3 days.
Why does it work?
Muscles fibers are grouped in two categories, type I and type II.
Although all muscles contain both types of fibers, higher percentages of one or the other will be present depending on the
function of that muscle. In a normal muscle contraction, type I fibers are recruited first. Only when the effort increases
are the type II fibers recruited (Witjing & Freed, 2003). Therefore, what we find is that the low intensity exercises
used in early rehabilitation benefit primarily the type I fibers. Since the swallowing musculature has a higher percentage
of type II fibers, they are less affected by conventional rehabilitative exercises. ES reverses the recruitment pattern,
causing the type II fibers to contract first. Therefore, ES can effect a “re-training” of the type II fibers,
while voluntary exercises can improve movement and coordination as a whole. Since swallowing may occur over 2000 times
per day, functional gains through ES therapy are continually exercised and practiced, thus, solidified and maintained.
Current Research
Based on the findings of researchers such as Burnett et all (2003)
and Grill et al (2001), researchers of the Laryngeal and Speech Section of the National Institute of Neurological Disorders
and Strokes (NINDS) of the National Institutes of Health (NIH) are conducting experimental studies of the intramuscular application
of ES for swallowing disorders. As opposed to VitalStim therapy, in which the electrodes are placed on the surface of the
skin, intramuscular stimulation inserts the electrodes into the actual muscles. In dysphagia as a result of brain injuries,
in which muscles are no longer receiving appropriate signals from the brain, direct insertion of electrodes into the muscles
has shown to produce similar laryngeal elevation to that which is seen in a normal swallow (Burnett et al, 2003). This is
something that has not been elicited through VitalStim therapy (Freed et al, 2001).
The goal of this study is to “determine the feasibility of using extrinsic laryngeal muscle stimulation
to elevate the larynx in a manner that occurs during normal swallowing in patients with chronic dysphagia”, as well
as to determine “whether laryngeal elevation will assist with opening the upper esophageal sphincter for entry of the
bolus into the esophagus” (Humbert & Ludlow, 2004). The long-term goal of this study is to develop a laryngeal
neuromuscular prosthesis, which would consist of implantable electrodes and a push-button controller that would deliver stimulation
to the laryngeal muscles during swallowing. To be included in this study, patients must be between the ages of 18 and 80 with
chronic pharyngeal dysphagia secondary to neurological deficit (e.g., stoke, TBI, Parkinson’s disease).
Multimedia examples:
Feeding Strategies:
1. Positioning
Positioning is very important when
dealing with an individual with a feeding/swallowing problem. This is no different when working with a child with cerebral
palsy. The basic goal for positioning of an individual is to encourage a safe and pleasurable eating experience for
the child and the caregiver. Children with cerebral palsy frequently have decreased postural control which
exacerbates their swallowing/feeding problems. According to The Source for Pediatric Dysphagia, there are 3 distinct
postural functions that must be met for the child to be able to eat and drink in a normal manner. The first step is
postural activity. This activity requires us to look at how the body works from a developmental prospective. Postural
activity involves the different developmental stages the child goes through involving coordination and control of movements.
Next we look at postural control. This activity is important for the coordination of respiration and phonation.
Children with CP have problems with postural control due to the involvement of their muscles in the disease. Lastly,
it is important that the child develops postural alignment which is necessary for efficient and safe feeding/swallowing.
Children with CP have problems with alignment and stability of their
oral structures as well, due to their abnormal muscle tone and movement patterns. In order to achieve proper oral functioning
for feeding it is important to gain better head stability and to improve jaw control. The whole body plays a part in
proper postural alignment because head stability is dependent on trunk alignment, which is influenced by the stability of
the pelvic area. In order for the child to have good postural alignment they must have: neutral head flexion,
neck elongation, stable depressed shoulders, trunk elongation, a neutral base at the pelvis, and 90º hip flexion with
feet on a stable surface for weight bearing.
The most safe and effective position for feeding is an upright position
that incorporates the use of the chin tuck. This position helps promote the movement of food safely from the mouth through
the pharynx and into the esophagus and away from the airway. This position is also good to help improve the suck and
swallow of an infant because it gives more support for the mandible. Maintaining this head position for children with
CP is difficult due to their muscular control.
When dealing with an infant one needs to help position the child this
way. With bottle fed infants the position that is most common is feeding the infant on your lap. The feeder helps
maintain the infant in an upright position with their arm and body. It can be helpful if the feeder has a box or footstool
to place their foot on which will help decrease the infant’s hyperextension.
There is an exception to this rule of upright
positioning for feeding. For bottle fed children who have poor head control, poor lip closure and tongue thrusting,
it may be beneficial to feed them at a slightly inclined position. While this position may be helpful for feeding these
children it does increase the risk of aspiration because it makes it harder for them to control the food bolus. Due
to this fact, once the child is past bottle feeding it is important to find an alternative seating system that will help with
their postural alignment.
Tumble Forms® Feeder Seat - See image at bottom of page.
While there are many kinds
of adaptive seating devices available on the market, such as the Tumble Forms® Feeder Seat and the Snug Seat®, these products
are usually quite expensive. Since children grow so fast, this may not be the best route to go in all situations.
Many times towels or wedges can be used to help modify the child’s positioning for optimal feeding posture. Many
families have reported that the adaptive seating they were provided with only added additional stress and aggravation to the
feeding experience with their child and after a while they just stopped using it all together. This indicates that finding
the appropriate adaptive device will vary from child to child and may take time to find just the right one.
Once the appropriate seating is selected, it is important to position them in the ideal sitting posture for eating.
This position would be with their hips, knees and feet to be at a 90º angle with their weight equally distributed.
To help achieve this posture it is often necessary to use seat belts in the chair this will help stabilize the pelvis.
The table or tray of the chair will also help the child maintain the proper body alignment. Since one of the goals is to make
eating pleasurable the feeder should be positioned in a way that they can make good eye contact with the child and this makes
the interaction more natural.
2. Altering Textures
When an individual is having
difficulty with swallowing and are at risk for aspiration, many times it is necessary to alter their diet. Sometimes
the problem may be with a liquid bolus. In this case if an individual is having problems with a thin liquid they may
be moved up to thicken liquids of a nectar or honey thick consistency. Some individual’s will do this by drinking such
things as tomato juice, V-8 juice, or buttermilk that naturally has a thicker consistency. Other individuals use products
that are on the market for thickened liquids which include pre-packaged juices and water that have been thickened to a nectar
or honey thick texture. There is also a thickening mix that can be added to the individual’s beverage of choice to thicken
it to the desired consistency.
If the problem is with bolus formation or aspiration of their
regular diet, this too can be altered. The next level down from the regular diet would be one that appeared almost regular,
except hard, crunch or sticky foods are avoided. The mechanical soft diet is the next level, this is where the foods
are moist and have a soft texture, but they are still cohesive in nature. If this diet does not work then the individual
moves on to a pureed diet where the food is blended smooth and has no lumps. This diet can be done by simply pureeing
the foods in a food processor and some catalogs offer molds for the food to make them appear more appealing to the individual.
Additional information about products for altering diets can be found at http://www.novartisnutrition.com/us/productList?step1=hc&step2=81 .
If the individual is demonstrating poor oral control it may be necessary
to try thickened liquids. If they are showing signs of a delayed pharyngeal swallow try putting them on a thick puree.
When there is reduced laryngeal closure it may be necessary to try a thicker consistency than they are presently using. A
purred diet is often recommend for those individuals who experience difficulty in the oral preparatory phase of the swallow,
those who pocket food, and those who have pharyngeal retention of chewed solid food. Children with CP are usually
able to manage a solid bolus of food easier than a liquid bolus due to their poor lip closure and tongue thrust. Also,
they are more able to control a small bolus of liquid easier than they can a large one. It may be beneficial to introduce
more solid based foods to help improve tongue lateralization and help with up and down jaw movement.
For an infant who is experiencing a delayed swallow you can try very
cold formula or thickened foods that are very cold. One way to help coordinate the sucking for an infant is to have
them suck on a frozen pacifier. You can also help the infant control the bolus by using special nipples and bottles
that will let you determine the size of the bolus the infant is receiving.
With children, new textures should be introduced gradually. It may
also be beneficial to not introduce a new taste and a new texture at the same time. Instead provide the child with the
new taste in the texture they are accustomed to first then introduce it in a different texture at a another time. Just
as you go through different stages with a normal developing child’s diet as they grow this process is also needed for
a child with a swallowing/feeding disorder.
3. Eating Aids
Children who experience difficulty
when eating may benefit from certain eating aids that are on the market. These aids could include such things as special
bottles/nipples, cups, or eating utensils. These devices can help ease some of the difficulty of feeding time by just
making things easier for the caregiver and child.
A bottle that is good for a child with a weak suck is the Playtex®
Nurser. The outside of the bottle is made like a hard shell, while the inside of the bottle is like a small plastic
bag. The plastic bag is what you would place the liquid in. For the child with a weak suck you can gentle press
on the bag which will help the infant get the liquid out.
Bottles that have angled necks can also prove beneficial for these
infants because it helps to keep the neck in a slightly flexed poison while they are sucking. These bottles are also
good for infants who require feedings while in a prone or side-lying position. These bottles can be found in all baby
supply stores. The Volu-feed® bottles are also good for infants who may need the feeder to provide additional check
and lip support. This bottle is small and only holds 2 ounces and can be held in one hand.
As the child gets older and moves from the bottle stage and transitions
to using cups the need to find one that will best aid them while drinking. One of the best cups are ones that are designed
with part of the top cut out so the individual can drink without excessive neck flexion.
Flexi Cut Cups - See image at bottom of page.
Another cup that might be beneficial to use with the child is the
Infa-Trainer® Cup. This cup is good to use because you are able to set the slow rate of the liquid. This way you
can set it so the child is not getting too much liquid with each sip.
For children with feeding/swallowing problems it is also necessary
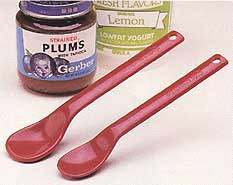
to find the right eating utensils for them to use. One of the most common feeding tools on the market is the Maroon
Spoons®. This spoon is good to use with children who have poor lip closure and tongue thrust. The design of the
spoon, which comes in two sizes, incorporates a very shallow bowl and it is made of a very durable material that is non-breakable.
Maroon Spoons® - See image at bottom of page.
There are also spoons on the market that can be put on the ends of
Z-Vibes® that allows the child to get oral stimulation while they eat. Textured spoons are also available where the
bowl of the spoon is shallow which allows the feeder to control the size of the bolus. The bottom of the spoon is textured
and supplies oral sensory stimulation while feeding.
For those children who can feed themselves, there are utensils that
are made for easy grasping.
These eating aids, just like any other equipment may not work for
all children. To ensure the safety and efficiency of the eating experience it may take some trials to decide which works
best for that particular individual.
Oral Motor Therapy
Oral motor therapy is a very beneficial tool to use with individuals
who have feeding/swallowing disorders. These techniques can help to facilitate more efficient motor tone, strength,
and mobility. Oral motor skills are developed in a progressive manner and can be beneficial for both speech and feeding
problems. Since we know that children with CP experience difficulty with lip closure, jaw tongue and tongue thrust this
therapy can help improve their oral motor skills.
There are many types of aids that can be used for oral motor therapy
to help the child such as blowing whistles and bubbles to help build coordination of the oral structures. Sensory awareness
issues may be addressed using massage, vibration, and mouth brushes using a NUK® brush.
It has proven to sometimes be beneficial to incorporate these oral
motor exercises or techniques right before feeding time. Many researchers have found that it is better to incorporate
therapy in this way because it directly correlates to each other. It helps show the functionality of the exercises instead
of only doing them in isolation. This means that right before the child eats the feeder would help “wake-up”
the child’s oral sensations by using massage, brushing or chewing tubes. This can prepare the child to be more
aware or their senses and ready to accept the bolus into the oral cavity.
When feeding the child during oral motor therapy there are different
ways to present the food that can help with the intake. If a child is having problems taking food from the spoon because
of tongue placement you can help present the food in the appropriate manner. For this task, place a small amount of
food on the spoon and present the spoon to the middle of the child’s tongue. Once the spoon is the proper position,
push down quickly on the tongue. This pushing down on the tongue will help the tongue muscles to push back. This
will help make the tongue move in an upward movement instead of the tongue thrust that is many times displayed.
If the child has problems with lip closure it may be necessary for
the feeder to aid in the support of the lip and jaw. This support can be offered by putting the index finger above the
top lip, the middle finger below the bottom lip and the ring finger under the chin. This assistance can be faded once
the child is able to master the coordinate and strength to support the lip and jaw adequately. Then the food is presented
in the same way that is described above because this technique also helps to facilitate lip closure.
It may be necessary to try different spoons to find the one
that works best for that individual child. The spoons vary in size and it may take some time to find the one that is
the appropriate size for that child. If the spoon is too big, or too much food is presented at a time this may be a
problem, especially if the child has problems with gagging. This helps to demonstrate that appropriate utensils and
food placement can make a difference in feeding.